E³ - Advanced Course: Gynaecology/Genitourinary Imaging
E³ 432 - Prostate cancer: a multidisciplinary approach
Lectures
1
Chairperson's introduction
05:00Anwar R. Padhani, London / UK
2
Oligometastatic prostate cancer (OMPC): opportunities for advancing care
15:00Thomas Zilli, Geneva / CH
3

Conventional versus next-generation imaging for detecting and directing MDT
20:00Irene A. Burger, Zurich / CH
4
Pokemets, biases, and follow-up after MDT
20:00Stefano Fanti, Bologna / IT
5
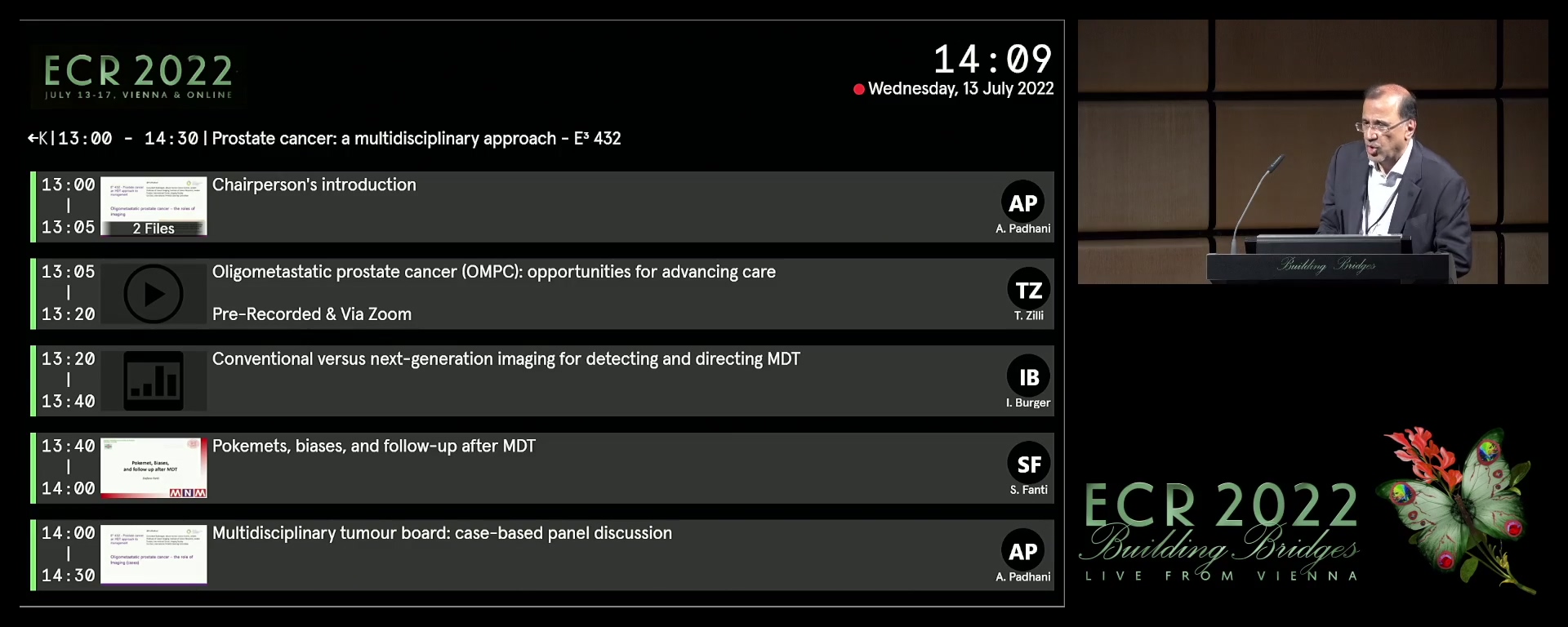
Multidisciplinary tumour board: case-based panel discussion
30:00Anwar R. Padhani, London / UK